The following is an example scenario.
Margaret, 74, was discharged after a cardiac procedure. Her daughter Linda, 47, managed the hospital stay. Her brother David, 52, lives in Denver. Her sister Rachel, 44, lives in Boston.
The coordination problem
David called Linda three times the day of discharge. Rachel called twice. Each call started with "so what exactly happened." Linda repeated the same update four times while trying to organize medications, schedule a follow-up, and get Margaret settled at home.
Nobody had been assigned to pick up the prescriptions. It turned out nobody had done it. Linda drove back to the pharmacy at 9pm.
The first week was functional but exhausting. Linda was the single point of contact for everything. David and Rachel felt helpful when they called. Linda felt more burdened after every call.
What changed
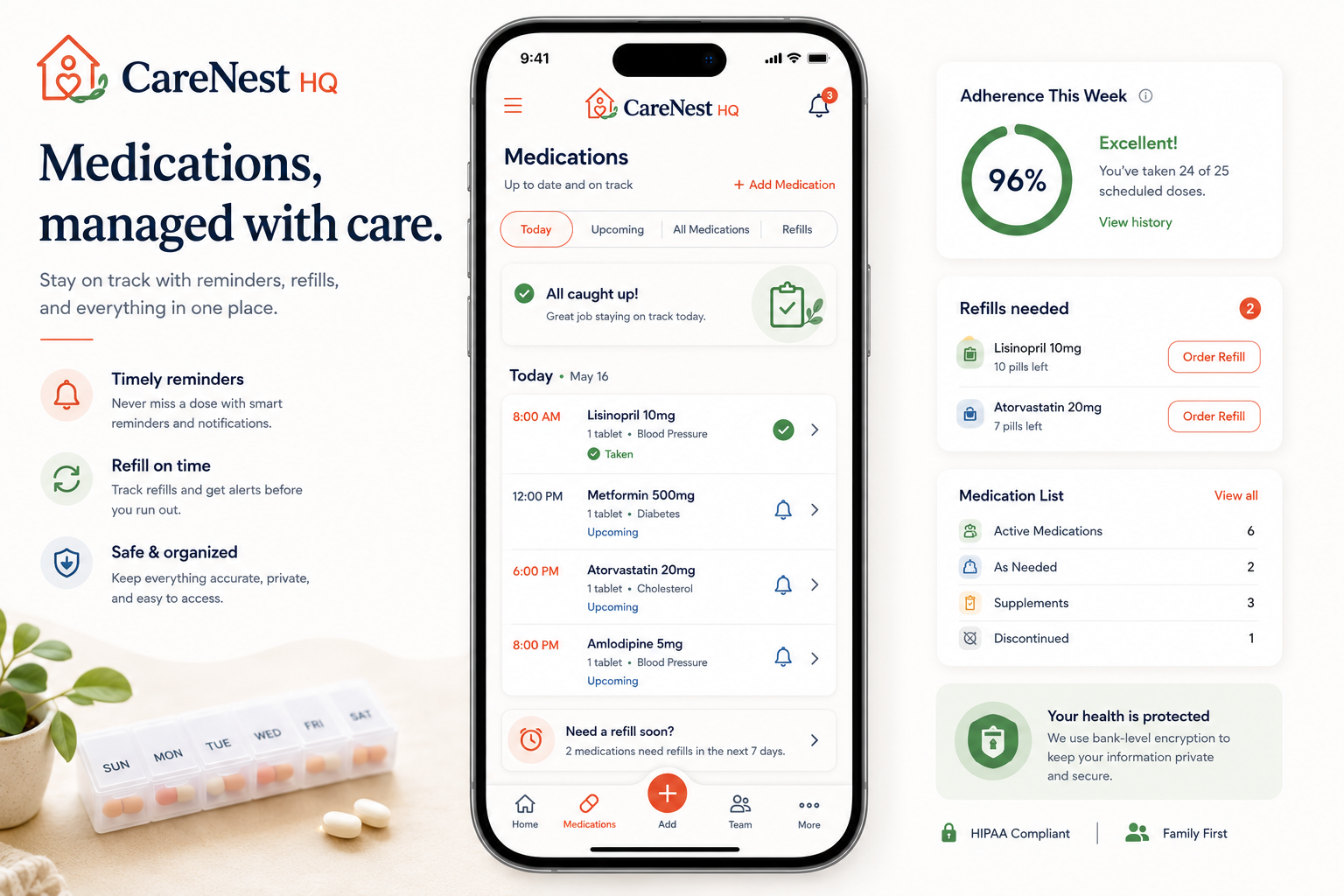
Linda created a CareNestHQ account and invited David and Rachel. She uploaded the discharge summary, set up the medications, and posted one Care Update covering what happened and what came next. She assigned tasks: David took insurance coordination by phone, Rachel took follow-up scheduling, Linda managed the day-to-day care.
The realistic outcome
The calls did not stop. But they changed. Instead of "what happened," the calls became "I scheduled the cardiology appointment, it is on the calendar." Instead of repeated updates, there was one shared record that David and Rachel could check without calling Linda.
Linda was still the primary caregiver and the hardest-working person in the family's care arrangement. But she was no longer the only person who knew what was going on. That was the difference.